The development of nutrition policy in Canada in the 1920s
Michael 2006;3:28–46.
Summary:
In the 1920s in Canada, the Federal Government’s Division of Child Welfare issued the nation’s first dietary guidelines aimed at encouraging women to breastfeed and also, somewhat ambivalently, encouraging women to feed cow’s milk to babies over nine months of age. The early 1920s was a time of transition in milk processing and distribution. Some cities and provinces had strong sanitary hygiene laws to ensure that milk was free of disease and contamination but others did not, so that general national guidelines promoting the use of cow’s milk were problematic.
These guidelines were promulgated at a time when many public health officials had begun to shift from vilifying milk, because of its potential to harbour dirt and bacteria and because of its well known links to infant mortality, to extolling its virtues because of its newly discovered rich vitamin and mineral content. The shift in milk’s status as an unhealthy liquid to the quintessential protective food for children, both in the public’s mind and in the mind of many public health practitioners, particularly those from cities that had managed to clean up their milk supply, was rapid and occurred while much the nation’s milk supply was in fact not safe. The promulgation of dietary guidelines promoting the consumption of cow’s milk for babies over nine months at this time was inconsistent and likely quite dangerous, particularly as Canada during the 1920s had the highest infant mortality rates in among industrialized nations.
The guideline was issued at a time of scientific enthusiasm over the new value of milk in protecting against under-nutrition and promoting optimal health. The dairy industry and the Federal Department of Agriculture unabashedly promoted the protective benefits of milk in large national campaigns overwhelming the ability of the Division of Child Welfare to deliver the best possible dietary guidelines for the times.
The relatively weak guidelines developed by the Division in the 1920s demonstrates how, in the absence of a strong nutrition policy centre, inappropriate and perhaps unhealthy nutrition advice was too easily modified by the dairy industry and it’s representative in the federal government, the Department of Agriculture.
Introduction
In 1921 the Division of Child Welfare in the Federal Department of Health developed Canada’s first national dietary guidelines in an attempt to improve breastfeeding habits and encourage mothers to feed their babies more cow’s milk (Canadian Mothers Handbook, 1923). These dietary guidelines were developed primarily to reduce infant mortality rates and, not surprisingly, given the well known contribution of milk to these persistently high rates, the guidelines were ambivalent in their advice about the consumption of cows’ milk.
The Division of Child Welfare’s guidelines were developed during a transition time in the history of milk as it emerged from its long held status as a food easily contaminated and a dangerous carrier of diseases of infancy and childhood to its new status as the premier protective food for children containing life enhancing vitamins and minerals (Dupuis, 2002). This transition occurred during the 1920s in a Canada covered with a patchwork system of municipal and provincial sanitary hygiene laws so that milk was clean and disease free in some cities and in some regions but not in others (Davidson, 1949; Curan, 1954; MacDougall, 1990). It was also a time of transition for the dairy industry which, in the face of declining dairy exports and domestic milk consumption, turned increasingly to public health professionals and nutritionists to increase sales, in particular of fluid milk by changing the status of milk from an unhealthy to a healthy food.
The breastfeeding guidelines developed by the Division of Child Welfare were widely disseminated to the general public in the inter-war years with the publication of the highly popular Canadian Mother’s Books (Canadian Mothers Handbook, 1923). Paradoxically, wide dissemination of this advice occurred as breastfeeding in Canada, and the most of the rest of the developed world, began an historic and profound fifty year decline which was only reversed in the late 1960s (Myers, 1981). This occurred as the medical profession in Canada consolidated control over medical practice and as it increased it’s over sight over pregnancy and birthing, in part because of growing public concerns over sustained high maternal mortality rates during the inter-war years (Kerr, 1935; Coburn et al, 1981).
A study of the Division’s guidelines and the circumstances of their introduction and widespread dissemination provide insight into what was the first nation-wide attempt at nutrition policy making in Canada and elucidates the complex interplay of health beliefs, public health, economics, and politics in developing Canada’s first nationally promulgated dietary guideline.
The general purpose of this paper is to describe Canada’s first foray into the development of national dietary guidelines. Besides this purely descriptive task the paper seeks to elucidate and explain the interplay of economics, science, and public health that shaped these early dietary guidelines and extract lessons that may be relevant to nutrition policy making today.
Breastfeeding and doctors in Canada in the 1920s
There is a long history of artificial feeding from ancient times up to the development of modern public health legislation, which shows that this form of feeding, in unsanitary conditions, generally meant death for an infant (Baumslag and Michels, 1993; Fildes, 1986; Stuart-Macadam and Dettwyler, 1995). Artificial feeding of infants in cities undergoing the transformation of an industrial revolution, such as occurred in Canada towards the end of the 19th century and in the early 20th century, was a dangerous practice as it brought babies into direct contact with contaminated, often germ ridden, water and cow’s milk (Ward and Ward, 1984).
There is some evidence, particularly in North American cities, where wet nursing was not as popular as in Europe that the rate of artificial feeding among poor women increased quickly in the late 19th century (Fildes, 1998). It is likely that poor urban women in the difficult working conditions of the time may have had particular difficulty in sustaining breastfeeding. At the same time, these poor women would have faced unsanitary living and difficult working conditions and, if they used artificial feeding, access mainly to contaminated water and milk for their babies (Ward and Ward, 1984).
Public health reformers were well aware of this in the late 19th century. In Britain the scientific links between poverty, increased artificial feeding, and infant mortality were established by the turn of the century. In a classic study of infant mortality among the poor conducted in London at the turn of the century, Newman (1906) concluded that «a mother suckling her infant requires nourishment, and it is lack of nourished mothers among the poor- many of whom are half-starved- that leads to the inability to provide milk for their offspring. This, in its turn, leads to early weaning, which involves artificial feeding, which is one of the most difficult undertakings in the tenement homes of the poor. And so it comes about that the earlyweaned infant is so often marked for death in infancy.» (Newman, 1906, p.260).
The links between artificial infant feeding and infant mortality were also well known in Canada (MacMurchy, 1923). The industrial revolution and concomitant social upheavals underway in Canada in the 1880s and 1890s provoked increasing pressure for social reform spearheaded by organizations such as the National Council of Women, the Women’s Christian Temperance Union, and the Social Service Council of Canada. These and resulted in the establishment of milk depots in some Canadian cities and Child and Maternal Hygiene Divisions in many municipal public health departments which educated women to breast feed their infants (Allen, 1971; Moscovitch and Drover, 1987; Valverde, 1991).
The social reform movement in Canada achieved much by World War One, including the development of public health legislation in many provinces and municipalities, and, at the federal level, created the political pressure to establish a national department of health including a Division of Child Welfare. However, by War’s end this movement was largely spent as a social force for change (McCuaig, 1980). The 1920s was a time of growing public faith and belief in the power of science in general and increased respect for the achievements of medicine in particular as the medical profession became increasingly better trained, better able to effect cures, and as the profession grew in stature and organizational power (Coburn et al, 1981).
However, many in the medical profession did not view breastfeeding in a positive light. For example, in the earliest Canadian medical investigation of breastfeeding among 370 children attending the Nutritional Clinic at Toronto’s Hospital for Sick Children investigators claimed that malnutrition cases were to be found in equal proportion among breast fed and bottle fed babies (Macdougall, 1922). According to the investigator, the cause of malnutrition in approximately half these cases was due to mismanagement and «lack of discipline in the home». In particular, «the first evidence of lack of home control is the fact that the child nurses 15 to 18 months. When the parent fails to control a child of that age, what success need one expect in dealing with this same child at 10 years of age?» (Macdougall, 1922, p. 28).
This early medical study of breastfeeding illustrates the distrust the Canadian medical profession displayed towards mothers in general and breastfeeding in particular. The medical profession gained more control over the process of pregnancy and birthing in Canada in the period from 1920 to 1950. For example, by 1939, 41 % of women birthed in hospitals increasing to 67 % in 1949 (Burns, 1967). During this time, the advice dispensed by doctors to women increasingly promoted artificial feeding and diminished the importance of breast feeding.
As Myers as shown, during the 1920s middle class women moved away from breast feeding for many reasons. For middle class women, increasing public faith in science and therefore the science-based feeding increasingly promoted by doctors, and the need for more independence for middle class women made artificial feeding more appealing (Myers, 1981). Thus, at the very time when national nutrition guidelines were developed and widely disseminated to promote breastfeeding, new medical and social conditions were leading to a profound decline in breastfeeding and increased exposure of very young infants to cows’ milk.
The availability of disease free cow’s milk in Canada in the 1920s
During the latter quarter of the 19th century and the first two decades of the 20th century, rapid industrialization and consequent separation of farm from the urban table, stretched the primitive storage and distribution systems of the day rendering milk an even greater hazard for poor urban children than it had ever been on the farm (Cohen and Heimlich, 1998). Milk had to be transported long distances and stored for relatively long times in the absence of refrigeration and it was often obtained from tuberculosis infested cattle living on un-inspected farms and unsanitary dairy barns (Dormandy, 2000).
This began to change in Canada, beginning in Toronto, which passed laws as early as the 1880s to regulate the dairy barns within the city (Mac-Dougall, 1990). By 1908 Ottawa passed stringent by-laws requiring the inspection of all cattle supplying milk to the city in an attempt to extend its dairy inspection regime to it’s rural milk shed (Hollingsworth, 1922). Toronto passed similar laws at this time and with growing pressure, in 1911, Ontario passed its Milk Act mandating the inspection of herds and dairy facilities province wide. In 1914, in a further effort to clean the milk supply, Toronto city council passed legislation making pasteurization of all milk sold in the city compulsory so that by the early 1920s milk in Toronto was probably safe (MacDougall, 1990).
The first state-level legislation in North America making pasteurization of milk compulsory was passed in Ontario (as amendment to the Public Health Act) only in 1938. During the 1920s and 1930s only «fifty municipalities of the eight hundred in the province had passed by-laws requiring the pasteurization of all milk offered for sale» (McHenry, 1941). As late as 1922, the head of the National Dairy Council of Canada told a meeting of the Canadian Public Health Association that, «milk sold in Ontario for domestic consumption (that is outside of our larger cities), is disgusting, dirty and dangerous» (Stonehouse, 1922a, p.298). In an article in the Public Health Journal he warned that the Council required continuing education of farmers, milk processors and distributors, and greater inter-cooperation between producers and medical officers of health to maintain current standards and further improve the cleanliness of milk (Stonehouse, 1922b).
Even in Canada’s most activist public health province through the 1920s and 1930s the milk supply was uneven in its cleanliness. And, outside Ontario, provincial legislation and most municipal by-laws were not as advanced. For example, in Canada’s largest city (at the time) Montreal, milk was not safe as evidenced by continuing milk-borne typhoid epidemics through the 1920s (MacDougall, 1990).
Thus, in spite of better legislation in some regions, greater awareness within the milk industry, more inspection of cattle and dairy facilities, and greater acceptance and availability of pasteurized milk, much of the Canadian milk supply was unclean and potentially dangerous during the 1920s and 1930s.
Reforming milk’s image
While most public health professionals had spent the last quarter of the 19th century vilifying milk and warning the public of its dangers by the early 1920s, at least in cities where the milk supply had been cleaned up, these same professionals began to extol the virtues of milk. Why this about face?
This came about mainly because of the discovery that besides fats, protein, and carbohydrates, vitamins and trace minerals also were necessary to sustain life. These discoveries came quickly between the turn of the century and the early 1920s (Nestle, 2002). Foods rich in vitamins were dubbed «protective» and milk was quickly identified as the most ideal protective food because of its high energy, mineral, and vitamin content (Valverde, 1991).
As well, milk had a special place in early vitamin research. When researchers broke food down into protein, fat, and carbohydrate and fed these constituents in pure form to baby animals they died. But, when fed milk these animals thrived. They used milk as they knew that as nature’s food for young animals it contained all the elements necessary for life. And, it was, in many cases, from milk that these researchers had isolated the first vitamins (Rosen, 1958).
The publicity around these early vitamin studies was enormous. The role of milk in these experiments was as also well publicized and provided milk with a new image. Following the vitamin discoveries public health professionals were divided about the impact of pasteurization of cows’ milk as some felt this would denature the vitamins negating milk’s positive impact on health (Hollingsworth, 1922). Once, it was discovered that pasteurization only minimally affected vitamin content public health professionals realized that combined municipal regimes of farm and dairy inspection and pasteurization would make milk safe and once safe, an ideal protective food.
Thus the early 1920s was a transition time for milk. On the one hand, because of the uneven cleanliness across the milk supply it was still dangerous but, on the other hand, it was becoming quickly known as the ideal protective food, particularly for children. In order to understand how Canadian health authorities in the 1920s developed guidelines based on feeding cow’s milk to babies, children, and pregnant women it is necessary to consider the position and the needs of the dairy industry at this time as the 1920s was also a time of transition for this industry as it faced new challenges.
The relationship between the federal government, the dairy industry, and public health officials in the 1920s
In the last quarter of the 19th and first quarter of the 20th century the dairy industry in Canada was overwhelmingly concentrated in the provinces of Ontario and Quebec. The factory system of cheese production, developed in nearby New York State in 1850, had made its way to Canada by the early 1860s and by the late 1860s there were over 235 cheese factories in the province of Ontario alone (Fowke, 1947). By the 1880s Ontario and Quebec had developed a sophisticated export oriented cheese and butter factory system with most exports destined for the British market.
The development of cheese factories and creameries was encouraged by the federal Department of Agriculture through the office of the federal Dairy Commissioner established in 1890 (Fowke, 1947). During the last decade of the 19th century experimental agricultural stations were established across Canada to teach farmers and entrepreneurs the business of factory cheese and butter production. Through these experimental stations the department of Agriculture subsidized the construction of local factories and the training of personnel. Once these demonstration projects were established the department would withdraw allowing local businessmen to finance further operation and expansion* It should be noted that the Canadian experimental agricultural stations had a purely agricultural purpose unlike the stations established by Atwater in the United States during this same era (Aronson, 1982). In the last decade of the 19th century, Atwater firmly linked the emerging science of nutrition with the problems of efficient labour supply and labour harmony in the rapidly industrializing conditions of America at the time and used agricultural stations established by the USDA to pioneer the new nutrition science (Aronson, 1982). Conditions in Canada were very different at this time. Canada was a small nation, with a small economy and, relative to the United States, an immature industrial infrastructure. In Canada the science of nutrition remained, relative to the United States and Europe, under developed and under appreciated. As an example, in Canada it was only in the late 1930s that the first scientific dietary surveys were conducted whereas the first surveys in the USA were conducted in 1885 (Pett, 1944).. As well, in the 1890s as refrigeration systems developed, and became a key to the expansion of the export market for dairy products, the department of Agriculture actively subsidized the development of refrigeration storage facilities at key export ports (Britnell and Fowke, 1962).
By the turn of the century Ontario and Quebec had a sophisticated dairy industry (actively supported by the federal government) based on exporting cheese and butter mainly to Britain. Exports of cheese and butter peaked in the first decade of the 20th century and dropped thereafter as local populations expanded and farmers shifted from cheese to fluid milk production to meet this local increase in demand and as Canadian dairy exports in the British market faced increasingly stiff competition from New Zealand, Australia, and Denmark (Skogstad, 1987).
In Canada prior to the First World War the dairy industry remained remarkably un-concentrated. Fluid milk and butter production was mainly based on single family farms and while cheese production, with its need for factory facilities, required more capital, it also remained relatively un-concentrated. Concentration in the fluid milk distribution business varied by region and city. For example, in the year preceding the First World War the cities of Ottawa and Regina were served by one large distributor whereas Toronto had over 50 distributors (Report of the Milk Committee, 1917).
In 1917 towards the end of World War One, the federal government passed the War Measures Act and created a centralized Food Control system. In an effort to increase the efficiency of milk production and distribution on the home front, the Food Controller formed a Milk Committee which recommends consolidating the dairy industry, particularly its milk distribution component. The committee felt that fewer producers, suppliers, and distributors, would increase the economic efficiency of the system, ensuring that farmers obtained better prices and therefore better incentives to produce, and that the reduced number of distributors and producers would make it easier to organize effective systems of public health milk inspection.
While calling for increased consolidation in the milk industry, the federal Department of Agriculture spearheaded an increased drive for agricultural production specifically for export under the slogan «Patriotism, Production, and Prosperity» resulting in greatly expanded dairy capacity which peaked just as the war ended and export markets for dairy products dried up (Britnell and Fowke, 1962, p.48). The abrupt shift to dependence on domestic consumption of milk, butter, and cheese, at the end of the war, during a time of growing food price inflation, which restricted the ability of domestic consumers to purchase dairy products put the dairy industry into crisis .* Dupuis (2002, p.114)has shown that in the United States the dairy industry faced similar pressures at the end of World War One. The price of milk increased from 8.8 cents in 1914 to a high of 15 cents a quart in 1920 and for the duration of the decade hovered at 12 cents, approximately 40 percent higher than it had been at the beginning of the War (Dominion Bureau of Statistics Report, 1960) (Figure 1).
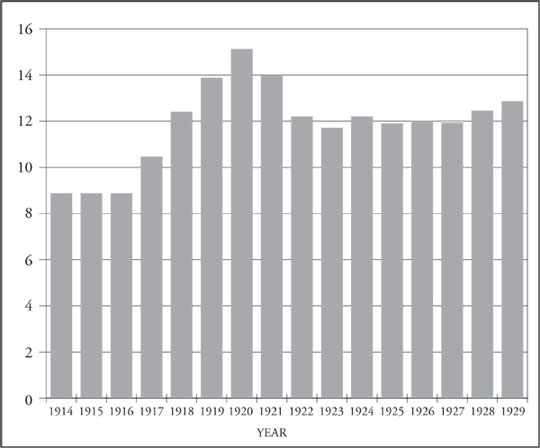
Figure 1: Fluid milk prices in Canada, 1914 to 1929 (cents per quarts).
The Food Controller’s Milk Committee reported that, «any slight increase in the price of milk, unfortunately, has been followed by a largely decreased consumption» (Report of the Milk Committee, 1917, p.6.). Milk consumption was clearly very sensitive to reductions in disposable income. Given the inflationary conditions at that time, the committee recommended that «a campaign of education be undertaken, emphasizing the relatively high food value of milk and the many ways of using it. Such a campaign could, perhaps, best be carried out by teachers of Domestic Science and by home economics Associations» (Report of the Milk Committee, 1917, p.6.).
This committee and the dairy industry clearly realized that the price elasticity for milk might be reduced if milk’s image could be reformed. The authors of this report understood that enhancing milk’s image would take more than a public relations campaign and suggested that the industry work more cooperatively with public health professionals to clean the milk supply.
The process of making milk supplies safe had often involved conflict between dairy farmers, processors, and distributors and municipal public health officers as the latter battled to regulate and to convince the industry of the dangers of dirty milk in spreading disease (Hollingsworth, 1922). The process of educating farmers, processors, and distributors and of cajoling industry into safer practices involved compromise as well as conflict, both within the industry and between public health and industry officials, so that in many cities by the end of the second decade of the 20th century, public health professionals and the dairy industry had a long history of working with each other.
For the first time in the history of the urban sanitary reform movement public health professionals began to recommend clean and inspected milk as the ideal protective food. As early as 1917, as shown by the report to Canada’s Food Controller, the dairy industry also began to campaign harder amongst its producers, processors, and distributors to improve the cleanliness of the milk supply and harness their relationship with public health officials, nutritionists, and dieticians to promote the protective benefits of milk to children.
An early example of this occurred in Toronto in 1922 in an extremely well publicized joint campaign by the Canadian Public Health Association, the Child Welfare Council, and the National Dairy Council of Canada. These groups sponsored Milk Week specifically targeting school children and their mothers to promote increased consumption of milk (Department of Pensions and National Health, 1923). The thrust of the campaign was that milk was vitamin and mineral rich with special protective effects on children’s health. The message was spread round the city by politicians, public health and National Dairy Council officials with speeches, carnivals in local parks, and parades so that it had an extensive reach.
As well, in 1923 officials from the Federal Department of Agriculture established strong alliances with the Federal Division of Child Welfare and national child welfare and women’s groups organizing several nutritionbased campaigns to increase the «use of milk for children and mothers» (Department of Pensions and National Health, 1923, p. 42). In 1926 the Federal Department of Agriculture’s, Milk Utilization Branch instituted a milk consumption promotion policy «cooperating with public health nurses and child welfare workers; assisting in provincial schemes, addressing dairy conventions meetings of school teachers and also public, collegiate and normal school classes». No opportunity is lost for disseminating information as to the dietary value of milk and its products.» (Department of Agriculture, 1926, p. 34). The Milk Utilization Service was engaged in «the work of increasing the consumption of dairy products by arousing public interest in their nutritional value» (Department of Agriculture, 1926, p. 86). By the late 1920s dieticians were «employed in this work, had booths for demonstration purposes at the leading exhibitions, attended meetings of health and child welfare organizations, women’s institutes, dairy conventions and other similar gatherings.» (Department of Agriculture, 1927, p. 40).
Although, particularly early in the 1920s, the cleanliness of the Canadian milk supply was uneven, public health professionals, the dairy industry, and the Federal Department of Agriculture increasingly joined forces to promote increased consumption of milk among children. For public health professionals working in cities with clean milk, given the recent discoveries of the vitamin and mineral content of the liquid (and at least 35 years before any hint of a pejorative association between the fat content of milk and ill health), this 360 degree change in attitude towards milk made good health sense. For the dairy industry, given decreasing milk consumption following the war, the emerging protective status for milk by the early 1920s was a marketing opportunity. However, as will be shown in the next section, for public health professionals attempting to generate nation wide dietary advice directed primarily at reducing infant mortality, the legacy from milk’s past was not so easy to jettison.
The division of child welfare and Canada’s first dietary guidelines
The Division of Child Welfare was formed in 1919 within the Federal Department of Health just one year after it was formed. The mandate of the division was to reduce the persistently high infant mortality rate in Canada (Schnell, 1987). In 1921 the infant mortality rate was 102.1 deaths per 1,000 live births. By 1929 the infant mortality rate was 92.9 per 1,000 live births, a reduction of approximately 10 % through the 1920s (Statistics Canada, 1991). This reduction was very small and the Federal Department of Health was also aware that rates, at that time and well into the 1940s, in Canada were the worst in the industrialized world noting that in 1921 the infant mortality rate in Canada was more than double that in New Zealand, which had the lowest rates among developed nations (Department of Pensions and National Health, 1924).
The gravity of this situation and the well accepted links between malnutrition, artificial feeding with cow’s milk, and infant mortality as well as the new information on the protective value of milk figured strongly in the Division’s first national dietary guideline directed to expectant and new mothers. These guidelines were first published by the Division in 1921 in the Canadian Mothers Book (CMB), in both English and French and disseminated widely across Canada through the 1920s (Department of Pensions and National Health, 1923).
The CMB reflected an ambivalence about milk as it gave general advice to pregnant women to use it as a protective food but, in its specific diets never actually instructed pregnant women to drink milk. And, the CMB issued dire warnings to mothers against the feeding of cow’s milk to babies less than nine months of age and strongly advocated breastfeeding for the mother as «she knows her nursing is the greatest safeguard for the baby’s life. She knows that her milk will not only nourish him but protect him from many of the diseases of infancy. She does not want her baby to die. Nursing the baby is the easiest way. No formula with bottles and rubber nipples, and measuring spoons and milk-sugar and sterilizing, and no one knows what else, for the Canadian Mother. These things will get dirty and dirt in milk is death to the baby.» (Canadian Mothers, Handbook, 1923, p. 72).
In fact the CMB advised mothers to drink cow’s milk only after her baby was born. The CMB advised women to «keep on the same diet that suited you before the baby came but drink a great deal more- say a pint or more of milk a day and plenty of water three or four times a day. You should have meat at one meal every day. Milk is our greatest protective food. You must have it.» (Canadian Mothers Handbook, 1923, p. 82).
Thus, new mothers were specifically advised to drink milk but pregnant women were not.
After clearly warning Canadian mothers away from feeding milk to babies less than 9 months of age the CMB described the role of cow’s milk in the diet of children once they attained 9 months as follows: «Milk is the indispensable food for children. They cannot do without it. The cow has been well called the «the foster mother of the human race.» Little children must have milk to enable them to grow properly. No matter what it costs, milk is still the cheapest food for children. Children from nine months to two years should have about two pints of milk every day in addition to other food, and it is really a mistake to give them any less till they are about twelve years of age. Three large cups of milk a day is the very least they should have» (Canadian Mothers Handbook, p. 107).
The CMB graphically and repeatedly advised that milk for babies over 9 months of age should be dirt free, pasteurized and stored properly, reflecting the extreme unease that professionals in the Division of Child Welfare felt, in the early 1920s, about the safety of the milk supply.
In speaking of the situation in the United States around the same time, Apple stated that «it is likely that the rising standard of living, greater access to medical care, and improved food and water supplies in the United States in the first half of this century at least in part masked the negative effects of the growing utilization of artificial infant feeding» (Apple, 1987, p. 172). Infants and children of women, particularly poor women, were vulnerable at a time when their mothers were moving away from the practice of breastfeeding under conditions of unavailability or sporadic availability of clean milk and water, and before the era of rapidly rising standards of living and widespread availability medical care.
The guidelines developed in the Canadian Mother’s Book, the first guidelines developed in Canada for nationwide dissemination, contained a stark inconsistency on the one hand promoting cow’s milk as «the» protective food and on the other hand, warning strongly that if used inappropriately it would kill the baby. This message, promulgated given the uneven availability of clean milk in the early 1920s in Canada, may have been more than inconsistent – it was likely quite dangerous.
Throughout the 1920s Canada had the highest rate of infant mortality among industrialized nations (Schnell, 1987; Statistics Canada, 1991, Department of Pensions and National Health, 1924). The rate of infant mortality did not begin a steady decline until the early 1930s. It is quite likely that a considerable portion of this mortality during the 1920s was due to continued ingestion of unclean milk during artificial feeding. It is likely that the cow’s milk promotion component of the CMB’s dietary guideline was unhelpful in this situation.
The guideline was issued at a time of scientific enthusiasm over the new value of milk in protecting against under- nutrition and promoting optimal health. The public’s enthusiasm for the new nutrition science, coupled with local public health promotion campaigns with clean milk, and the unabashed promotion of the protective benefits of milk by industry and Department of Agriculture officials, overwhelmed the ability of the Division of Child Welfare to deliver the best possible dietary guidelines for the times.
With the luxury of hindsight, the best possible dietary guideline for the times would have given very little or no attention to cow’s milk or continued the older public health stance towards milk, which was overtly negative, and promoted a longer period of breastfeeding, followed by a long transition from breastfeeding to solid food. Instead of developing such a guideline, the Division of Child Welfare, did, presumably what it could, given the political pressures it was under, ending up with a compromise – with which it was clearly uncomfortable – which was probably not in the best health interests of mothers and children in Canada at the time.
Lessons for nutrition policy making today
This paper demonstrates how, in the absence of a strong nutrition «centre» in the federal government (the Division of Child Welfare was formed only in 1919 and was entirely shut down during the middle of the 1930s), what Cannon and Nestle call «eat less» nutrition advice, implied in the Division’s breastfeeding guidelines, was too easily modified by the dairy industry and it’s representative in the federal government, the Department of Agriculture (Nestle, 2002; Cannon, 1987).
The federal department of agriculture has figured large in Canada’s history in part because the overarching objective of Canadian national policy in the 19th and early 20th century was to build a strong agricultural sector, particularly in the west where prior to the building of the transcontinental railway in the 1880s, the Canadian government was concerned with the threat of American expansion into the Western provinces. The thrust of agricultural policy after building the railroad was to settle the Prairie provinces and create a Western Canadian economy on a strong agricultural foundation while at the same time strengthening the mixed and dairy farming economy of central Canada (Anderson, 1966/67).
Expansion of livestock production and the dairy industry was a key to this policy which was threatened by milk surpluses and the shutting off of export markets for dairy products in the aftermath of World War One. In the early 1920s the objectives both of the dairy industry and national food policy makers in the department of Agriculture shifted to active promotion to increase the domestic consumption of fluid milk.
The new science of nutrition with its enthusiastic espousal of milk as the quintessential protective food was harnessed by these interests and new alliances made with public health professionals to garner their support to market milk, particularly to children. The nutrition professionals beginning to emerge from agricultural and home economics programs in the 1920s were employed by the federal department of Agriculture and the dairy industry to utilize the new science to promote increased milk consumption.* Nestle (2002) has demonstrated the same phenomenon in the United States around this time.
The alliance of agricultural interests and their successful harnessing of the new science of nutrition in the 1920s were so effective that they were able to market milk to children even in the face of clear evidence of high infant mortality rates which had been scientifically linked to the ingestion of unclean milk, in the absence of effective provincial public health legislation regulating the milk supply and, even though the price of milk was at historically high levels.
Within the federal government the only resistance to this enthusiastic food policy came from the Division of Child Welfare in the form of the nations first dietary guidelines warning mothers not to feed cow’s milk to babies less than 9 months of age. This resistance was half-hearted perhaps because the Division itself was also actively involved with the Milk Utilization program within the Department of Agriculture which specifically and aggressively promoted milk consumption among mothers and school children throughout the 1920s and 1930s.
Even as nutrition policy was emerging as a tool to fight the extremely high infant mortality rates of the 1920s it was overwhelmed by the already strong alliances formed between the federal Department of Agriculture and the dairy industry. Public attitudes about scientific progress, the promise of the new nutrition science, the needs of the increasingly powerful medical profession, and industrial and national interests promoting milk consumption dovetailed to overwhelm efforts to retard the promotion of milk to children and infants.
This historical study has relevance today. First, experts in the Division of Child Welfare promoted an indirect «eat less» message (at least for infants under 9 months of age) which would have acted to reduce the consumption of fluid milk (Nestle, 2002; Cannon, 1987). At the same time the Division was promoting milk consumption with its sister department, Agriculture in an alliance in which it was very much a weaker, junior partner so that nutrition policy was subordinate to food policy.
Second, this Division of Child Welfare’s nutrition message was promulgated with unequivocal evidence about the harm to health posed by drinking unclean cow’s milk. In other words, the evidence of harm was firm and uncontested. However, this secure scientific evidence was swept aside because of exciting new scientific developments attending the discovery of vitamins and because many of those in the public health community who had been involved in gathering and promoting the evidence of harm from unclean cows milk switched, as the milk supply became cleaner, to enthusiastic support for the new virtues of milk.
Today, nutrition policy makers are faced with the relatively new science of genetics which may be poised in similar fashion to overwhelm the more cautionary messages from the science of environmentalists and nutritionists opposed to genetic manipulation of the food supply. Health Canada has strong relationships with industry which could compromise its ability to generate nutrition advice which is contrary to industry interests. And, the move to harmonize nutrition standards with the United States, which has gained momentum over the past decade, will further restrict the independence of nutrition policy making in Canada in the near future and likely make Canadian nutrition policy more dependent on the needs of American food policy.
The switch in the 1920s from public health science’s vilification of cow’s milk to a position extolling its virtues cemented the alliance between the dairy industry and the federal government and shifted public attitudes towards milk. A key issue in today’s nutrition policy making environment will be the role which science, scientists, and scientific evidence plays in the nutrition policy making arena. Will the new science of genetics closely aligned, as was the vitamin science of the 1920s, with agriculture and agribusiness, similarly overwhelm the nutrition and health concerns of our time?
Acknowledgements
The support of the Social Sciences and Humanities Research Council of Canada is duly acknowledged. Ms. Nathoo holds a Trainee Award from the Michael Smith Foundation for Health Research. In addition Dr. Ostry holds a New Investigator award from the Canadian Institute for Health Research and a Scholar Award from the Michael Smith Foundation for Health Research. Dr. Dubois holds a scholar award from the Canadian Institute for Health Research and is also supported by the Canadian Institute for Advanced Research.
References
Allen, R. (1971) The social passion: religion and social reform in Canada 1914–28. (Toronto, University of Toronto Press).
Anderson, W. J. (1966/67) Canadian agricultural policy: a review. Occasional Papers on Credit, Livestock, Food Supply, (Ottawa, Policy No. 9, Agricultural Economics Research Council of Canada).
Apple, R D. (1987) Mothers and medicine: A social history of infant feeding, 1890–1950. (Madison, University of Wisconsin Press).
Aronson N. (1982) Nutrition as a social problem: a case study of entrepreneurial strategy in science. Social Problems. 29 (5) pp 474–487.
Baumslag, N. and Michels, D. L. (1993) Milk, money, and madness: the culture and politics of breastfeeding. (Westport, Connecticut, Bergin & Garvey).
Britnell, G.E. and Fowke, V. C. (1962) Canadian agriculture in war and peace 1935–1950. (Stanford, Food Research Institute, Stanford University Press).
Burns A.Y. (1967) The child and maternal health division of the Department of National Health and Welfare, Medical Services Journal of Canada. April pp.688.
Cannon, G. (1987) The politics of food. (London, Century Hutchinson).
Coburn, D., Torrance, G. M., & Kaufert, J. M. (1981) Medical dominance in Canada, in historical perspective: the rise and fall of medicine? International Journal of Health Services Research. 13 (3) pp 407–428.
Cohen, R. and Heimlich, J (1998) Milk: the deadly poison. (New York, Argus Publishers Inc).
Curan, R. E. (1954) Canada’s food and drug laws. (New York & Chicago, Commerce Clearing House Inc.).
Davidson, A. (1949) Food and drug administration in Canada. (Ottawa, Health and Welfare Canada).
Department of Agriculture (1926) Agriculture department annual report (Ottawa, Kings Printer).
Department of Agriculture (1927) Agriculture department annual report (Ottawa, Kings Printer).
Department of Pensions and National Health (1923) Health department annual report. (Ottawa, Kings Printer).
Department of Pensions and National Health (1924) Health department annual report (Ottawa, Kings Printer).
Dominion Bureau of Statistics: Price Division, Retail Prices Section (May, 1960) Urban Retail Food Prices, 1914–1959. (Ottawa, Queen’s Printer).
Dormandy, T. (2000) The white death: a history of tuberculosis. New York, New York University Press.
Dupuis, E. M. (2002) Nature’s perfect food: how milk became America’s drink. (New York, New York University Press).
Fildes, V. A.. (1986) Breasts, bottles, and babies. (Edinburgh, Edinburgh University Press).
Fildes, V. (1998) Infant feeding practices and infant mortality in England, 1900–1919. Continuity and Change. 13 (2) pp 251–280.
Fowke, V. C. (1947) Canadian agricultural policy: the historical pattern. (Toronto: University of Toronto Press).
Hollingsworth, J B. (1922) Milk and dairy inspection. The Public Health Journal of Canada. 43 pp 223–226.
Kerr, J. M. (1935) Need our mothers die? (Ottawa, Division on Maternal and Child Hygiene, Canadian Welfare Council).
Macdougall, C. S. (1922) Malnutrition in children of school age The Public Health Journal. 42 (3) pp.25–35.
MacDougall, H. (1990) Activists and advocates: Toronto’s health department, 1883–1983. (Toronto, Dundurn Press).
MacMurchy, H. (1923) Handbook of child welfare work in Canada, (Ottawa, Department of Health).
McCuaig, K. (1980) From social reform to social service. the changing role of volunteers: the anti-tuberculosis campaign, 1900–30. Canadian Historical Review. LXI (4) pp 485.
McHenry, E. W. (1941) Milk: the protected, protective food. Canadian Public Health Journal. 32 (4) pp 227–230.
Moscovitch, A. and Drover, G. (1987) The growth of the welfare state in the 20th century. In Moscovitch, A, and Alberts, J. (eds) The benevolent state: the growth of welfare in Canada, (Toronto, Garamond Press).
Myers, A. W. (1981) Breast-feeding: a Canadian perspective on a global priority. Canadian Medical Association Journal. 125 pp 1078–1142.
Nestle, M. (2002) Food politics: how the food industry influences nutrition and health. (Los Angeles, University of California Press).
Newman, G. (1906) Infant mortality: a social problem. (London, Methuen & Co).
Pett, L. B. (1944) Malnutrition in Canada. Canadian Medical Association Journal. 50 pp 9–14.
Report of the Milk Committee to the Food Controller for Canada: Including a Plan for the Re-organization of Milk Distribution. Food Controller for Canada (November, 24th, 1917) (Ottawa, King’s Printer).
Rosen, A. (1958) History of public health. (Baltimore and London, Johns Hopkins University Press).
Schnell, R. L. (1987) A children’s bureau for Canada: the origins of the Canadian council on child welfare, 1913–1921. In A. Moscovitch and Alberts, J (eds) The benevolent state: the growth of welfare in Canada, (Toronto, Garamond Press).
Skogstad, G. (1987) The politics of agricultural policy-making in Canada. (Toronto, University of Toronto Press).
Statistics Canada: Catalogue 82–549 Occasional (1991) Selected infant mortality and related statistics, Canada, 1921–1990. (Ottawa, Statistics Canada).
Stonehouse, E. H. (1922) A safe and clean milk supply. The Public Health Journal of Canada. 19 pp 449–454.
Stonehouse, E. H. (1922) The production of clean milk. The Public Health Journal of Canada. 21 pp 298.
Stuart-Macadam, P. and Dettwyler, K. A.. (1995) Breastfeeding: biocultural perspectives. (New York, Aldine de Gruyter).
The Canadian Mothers Handbook (1923) Dominion of Canada (Ottawa, Department of Health).
Valverde, M. (1991) The age of light, Soap, and water: Moral reform in English Canada, 1885–1925. (Toronto, McClelland & Stewart Inc).
Ward, W. P. and Ward, P. C. (1984) Infant birth weight and nutrition in industrializing Montreal. American Historical Review. 89 (2) pp 324–345.
Dept. of Health Care and Epidemiology
5804 Fairview Avenue,
Vancouver, BC
V6T 1Z3.
ostry@interchange.ubc.ca